Finger avulsion injurie
Case report
A 31-year-old female, working as a waitress in a café, suffered an accident at her workplace. The patient’s left index wedged into an orifice at the base of a refrigerator which she was trying to lift and move. This led to an avulsion of the second left digit and sub-amputation through the proximal interphalangeal joint (PIP) [Figure 1] with only an intervening cutaneous bridge remaining. The flexor digitorum profondus and superficial tendons were cut in Zone 2 and extensor tendon in Zone 4. There was no digital circulation. The case was defined as third stage according to Urbaniak classification. The patient was admitted to the hospital four hours after the accident.
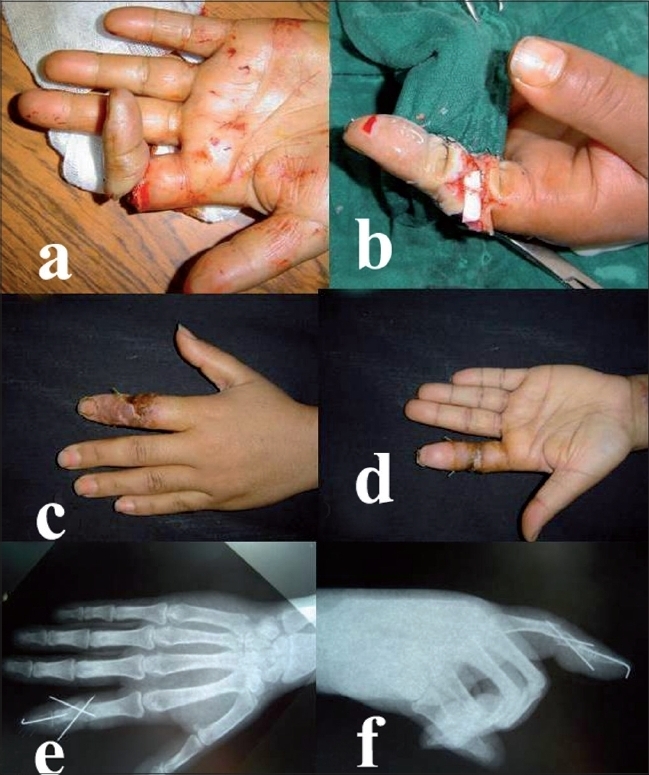
Figure 1
(a) Urbaniak Class III avulsion through proximal interphalangeal joint of left index finger with finger ischemia. Termino terminal anastomosis on the radial collateral artery after shortening arthrodesis of the proximal interphalangeal joint. Two weeks postoperative (c-d) aspect of the left hand after the procedure. Postoperative AP (e) and lateral (f) X-rays of left middle ray
The patient was taken up for urgent wound irrigation and debridment. The cartilage of the head of the proximal phalanx of the index finger (P1) was destroyed. A shortening arthrodesis of the PIP joint was performed at 15° flexion. The flexor digitorum profondus tendon and extensor tendon were sutured end to end. Peroperative examination revealed contusion of the nerve and thrombosis of the digital artery on the ulnar aspect. Arterial repair was performed by anastomosis of the collateral radial artery. The venous flow was restored by placing an interposition vein graft between two dorsal veins, harvested from the palmar side of the subcutaneous tissue of the wrist. The collateral nerve at the radial aspect was repaired by simple suture. The skin could be closed primarily by simple interrupted sutures as the soft tissues were lax due to the shortening arthrodesis of the PIP joint. During the postoperative period there was a slight marginal skin necrosis of a part of the dorsal surface skin which healed secondarily by ointment dressings. On follow-up one year later, the patient was extremely satisfied with the reconstruction. She had an active range of motion of 90° at the metacarpophalangeal (MCP) joint and good return of protective sensation.