Treatment and restoration of adult dentoalveolar trauma
Case report
A healthy 25-year-old woman visited our dental clinic 24 hours after an accidental fall. The physical examination revealed contusion of the lower lip, uncomplicated coronal fracture of all four upper incisors (Figure 1), and extrusive luxation of the upper right central incisor, which was also confirmed by the X-ray study (Figure 2). Alveolar fracture of the upper anterior buccal plate was identified by cone beam computed tomography (CBCT) (Figure 3) (1,3,4).

Initial intraoral view showing the coronal fractures of the incisors and extrusive luxation of the upper right central incisor.
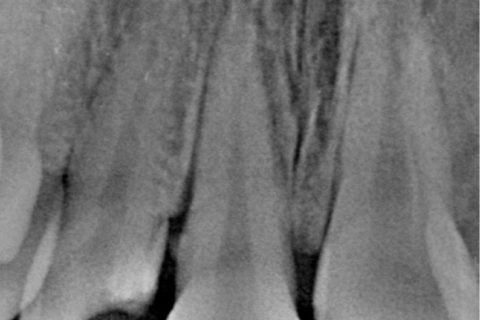
Periapical X-ray view of the upper central incisors, showing widening of the periodontal ligament of the upper right central incisor secondary to extrusive luxation.
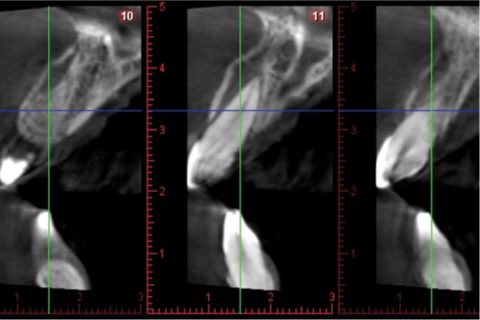
CBCT view showing of the upper central incisors, showing the alveolar fracture of the upper anterior buccal plate.
On the first visit and under local anesthesia, we repositioned the upper right central incisor within its socket, followed by splinting to the neighboring teeth with wire and composite material . Provisional reconstruction of the coronal fractures with composite was also carried out on the same visit. Antibiotic treatment was prescribed in the form of amoxicillin 875 mg and clavulanic acid 125 mg (Augmentine®, GSK,80 G, Brentford, Middlesex, United Kingdom), together with analgesia in the form of ibuprofen 600 mg (Normon, Madrid, Spain), during one week .
Three weeks later vitality testing using a tetrafluoroethane spray (Pharmaethyl®, Septodont, Saint-Maur-des-Fossés, France) yielded negative results with both upper central incisors and the right lateral incisor. Endodontic treatment of these teeth was sub-sequently carried out, with internal bleaching of the upper right lateral incisor using 35% hydrogen peroxide (Opalescence Endo; Ultradent, South Jordan, UT, USA), due to discoloration secondary to pulp necrosis. Internal bleaching lasted four weeks, after which composite veneers were prepared (Filtek Supreme XTE; 3M ESPE, St. Paul, MN, USA) for all four upper incisors in order to improve the esthetic outcome (Figure 4).

Provisional composite veneers of the four upper incisors.
Following stabilization of the clinical and esthetic condition of the patient, and after a 5-month waiting period, CBCT evaluation of the alveolar bone fractures confirmed healing of the buccal plate.
As final restoration, esthetic tests were made for the fitting of lithium disilicate veneers (IPS e.max Press; Ivoclar Vivadent, Schaan, Liechtenstein) on the four upper incisors. Preparation for veneers with a buccal thickness of 0.5 mm and a curved chamfer of 0.3-0.5 mm was carried out (Figure 5), followed by imprinting with triple-zero retraction thread (Ultrapak; Ultradent, South Jordan, UT, USA) and polyether (Impregum; 3M ESPE, St. Paul, MN, USA) as imprint material. The veneers were cemented using an adhesive technique (Variolink Veneer; Ivoclar Vivadent, Schaan, Liechtenstein), and resulted in a more natural smile (Figure 6 and 7).

Preparation for veneerson the four upper incisors.

Intraoral view of the porcelain veneers on the upper incisors.
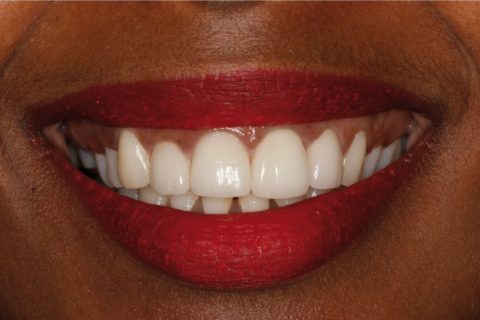
Extraoral view of the porcelain veneers on the upper incisors.
After two years the patient remains asymptomatic, with no signs of root resorption or ankylosis of the damaged teeth.