Earthquake injuries
Lei Liu, Gang Tan, Fujun Luan, Xin Tang, Pengde Kang, Chongqi Tu, and Fuxing Pei
The Wenchuan earthquake (May 12, 2008; 2:28 p.m. local time) was a disaster for China. Orthopedic surgeons faced major challenges in controlling fractures quickly and effectively, repairing tissue defects, closing the wounds, promoting wound healing, preventing infection, and minimising complications. Most of the patients brought to our clinic had severe open or closed bone fractures. The literature contains few reports of the effects of vacuum sealing drainage (VSD) combined with external fixation for patients who sustain fractures in these types of natural disasters.

Surgery
Thorough debridement was performed to remove contaminants and foreign matter and dead tissues. The length and alignment of the lower limb was restored by manual traction. Crush fracture bone grafts were performed first and were fixed with screws, gram needles, or wires. More than 5 cm from the fracture, the medial side of the tibia received external fixation pins, shelves, and fixed pressure. Patients with comminuted fracture and bone defects underwent traction using the healthy limb or the length of the fibula to assess restoration of limb length and mechanical axis, using the external fixator. Metaphyseal fractures involving knee and ankle underwent external fixation.

Fig. 2
Thorough debridement
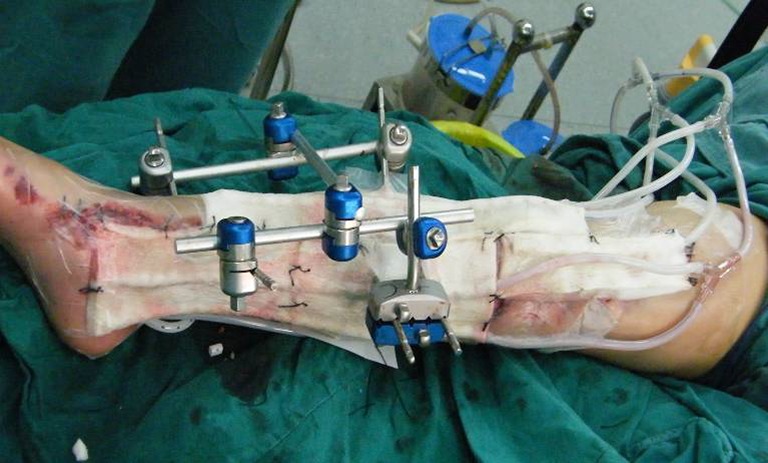
Fig. 3
The external fixation combined with vacuum sealing drainage (VSD) were performed after thorough debridement, and the VSD was linked to a negative pressure aspirator

Fig. 4
Secondary sutures were followed by treatment by external fixation combined with vacuum sealing drainage (VSD) until the wounds had healed well
After initial extensive debridement wounds were covered or filled with a Poly (vinyl alcohol) shrink formaldehyde bubble using 16 silica gel according to the wound size. The Poly (vinyl alcohol) shrink formaldehyde bubble was stuck to the healthy skin, and the wound was then closed with Poly amino acid ethyl ester films. In cases of multiple wounds, the wound drainage tube was connected through various links to the suction device (Fig. 5). Starting after drainage, suction was maintained at 40 kPa for seven to ten days of continuous negative pressure. During this period, no dressing changes were needed. Drainage into the negative pressure bottles was observed, as well as limb swelling, with regression of symptoms noted. After seven to ten days, the polyvinyl formaldehyde foam was removed, wound infection control assessed and a decision was made whether to proceed with granulation and delayed primary closure of wounds, skin grafting, or skin flap wound surgery. If infection was not well controlled, further debridement was performed. Negative pressure drainage was between 500 and 2,300 mL.

Figure 5.
Healing of the transposition laps