Intradural non-calcified thoracic disc herniation causing spontaneous intracranial hypotension: a case report
Michael Fiechter, Alexander Ott, Jürgen Beck, Astrid Weyerbrock & Jean-Yves Fournier
Case presentation
A 46-year old woman initially presented with progressive orthostatic headache (sudden onset) at the emergency unit since 1 month. There was no history of trauma and the neurological exam was normal. Analgesia and bedrest, as prescribed from the patient’s family doctor, had only minor clinical effect. Initial cranial computed tomography (CT) scan revealed small bifrontal hygroma. Pressure measurement by lumbar puncture was considered not reliable due to pressure values equaling to zero. Further workup by cranial and whole-spine magnetic resonance imaging (MRI; fluid-sensitive and thin-sliced) revealed cranial dural contrast-enhancement (with small bifrontal hygroma, Fig. 1a) as well as extradural fluid collection at the level of the thoracic spine suggestive of a dural leak causing CSF loss and thus SIH (Fig. 1b) [5, 6]. Three consecutive (unspecific) lumbar epidural blood patches (serially performed at 3 day intervals) were conducted without sustainable clinical amelioration.
Finally, a longspine CT-myelography (dynamic myelography with postmyelography spine CT imaging) identified a possible dural tear due to ventral extradural contrast leakage at the level of the thoracic vertebrae 11/12 and thoracic vertebrae 12 (Th12) / lumbar vertebrae 1 (L1) with high suspicion of a trans−/intradural lesion (Fig. 1c and d). Consequently, surgical exploration of the described levels was performed by a translaminar and transdural approach at the level of Th12 (Fig. 2a-d). Intraoperatively, a ventral dural slit was identified with CSF leakage to the extradural space at the level of Th12/L1 due to an intradural disc sequester (Fig. 2b). Subsequent resection of the disc sequester (by use of sensory/motor evoked potentials, SEPs/MEPs, of lower extremities and anal sphincter) with tight ventral/dorsal dural closure by suture (Fig. 2c) and laminoplasty of Th12 (Fig. 2d) was successfully conducted (refer to the intraoperative video animation in the “Additional file 1”).
Histological workup of the resected lesion confirmed non-calcified intervertebral disc material. The postoperative clinical course was uneventful. The patient underwent stepwise and cautious mobilisation to avoid relapse of CSF leakage. Immediate cessation of the orthostatic symptoms was observed postoperatively and at a 3 months follow-up and the patient was able to return to work. Conventional radiography of the thoracolumbar junction showed no signs of dislocation of the artificially reattached lamina of Th12. Written informed consent was obtained from the patient to report and publish individual patient data.
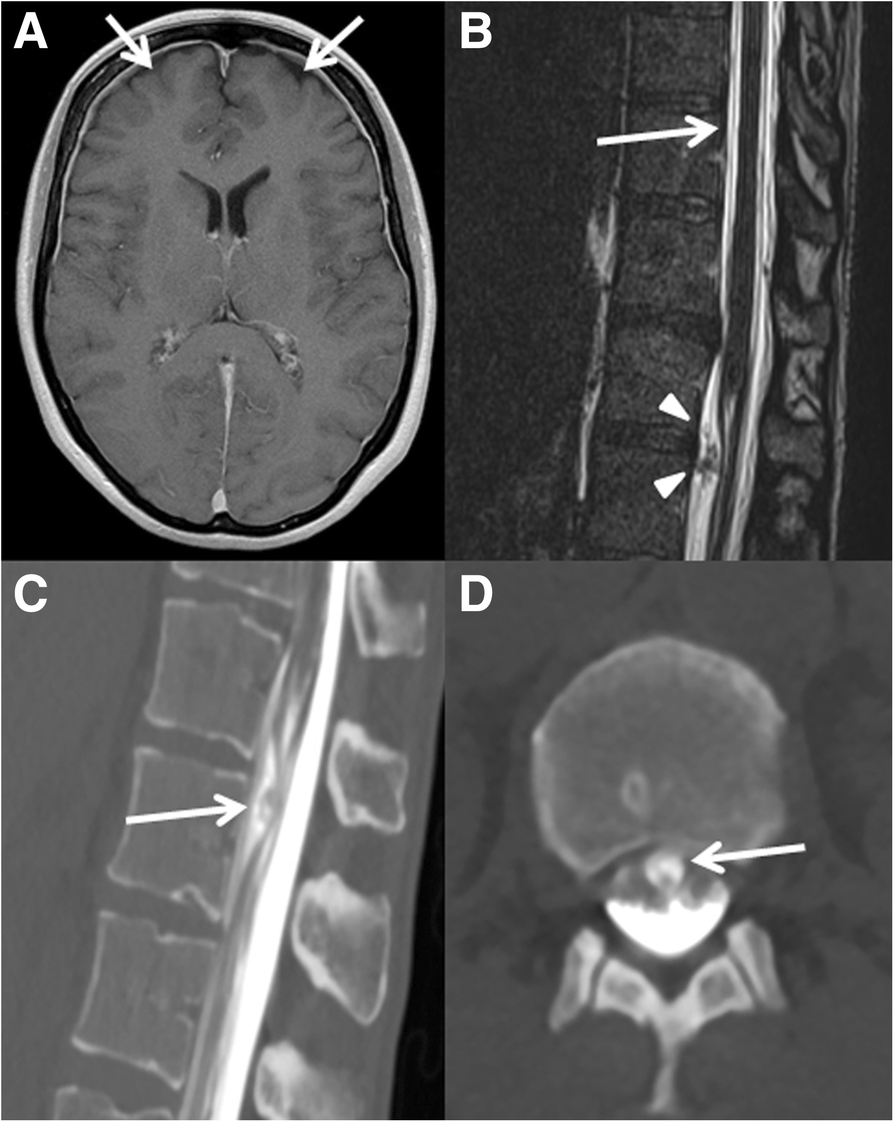
Figure 1. Diagnostic findings in a patient with spontaneous intracranial hypotension (SIH). Initial head-MRI revealed minor bifrontal hygroma (axial view, arrows) with diffuse dural contrast-enhancement as typical findings in a patient with SIH (Panel a). Subsequent whole-spine MRI (sagittal view) shows an extradural fluid collection (arrow) and an unidentified trans−/intradural mass lesion (arrowheads) at the level of thoracic vertebrae 12/lumbar vertebrae 1 (Th12/L1, Panel b). Finally, CT-myelography confirmed the suspected dural leakage caused by the unidentified trans−/intradural mass lesion (arrow) at the level of Th12/L1 (Panel c and d with sagittal and axial slices, respectively)

Figure 2.
Dorsal transdural approach and removal of an intradural non-calcified disc sequester causing a CSF leak. After laminectomy of thoracic vertebrae 12 (Th12), a dorsal dural opening was performed (Panel a). Subsequently, medial mobilisation of the spinal cord (under continuous intraoperative neurophysiological monitoring) revealed an intradural disc sequester at the location of the dural leakage (Panel b). After resection of the disc sequester, a water-tight ventral (and dorsal) dural closure was conducted (Panel c). Finally, dorsal dural closure and laminoplasty of Th12 concluded the intervention (Panel d)
References
- 1.Ducros A, Biousse V. Headache arising from idiopathic changes in CSF pressure. Lancet Neurol. 2015;14:655–68.
- 2.Schievink WI. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA. 2006;295:2286–96.
- 3.Cohen-Gadol AA, Mokri B, Piepgras DG, Meyer FB, Atkinson JL. Surgical anatomy of dural defects in spontaneous spinal cerebrospinal fluid leaks. Neurosurgery. 2006;58:ONS–238-45.
- 4.Beck J, Ulrich CT, Fung C, Fichtner J, Seidel K, Fiechter M, et al. Diskogenic microspurs as a major cause of intractable spontaneous intracranial hypotension. Neurology. 2016;87:1220–6.
- 5.Idrissi AL, Lacour JC, Klein O, Schmitt E, Ducrocq X, Richard S. Spontaneous intracranial hypotension: characteristics of the serious form in a series of 24 patients. World Neurosurg. 2015;84:1613–20.
- 6.Förderreuther S, Yousry I, Empi M, Straube A. Dilated cervical epidural veins and extra arachnoid fluid collection in orthostatic headaches. Neurology. 2001;57:527–9.
- 7.Schievink WI, Dodick DW, Mokri B, Silberstein S, Bousser MG, Goadsby PJ. Diagnostic criteria for headache due to spontaneous intracranial hypotension: a perspective. Headache. 2011;51:1442–4.
- 8.Mettler FA Jr, Huda W, Yoshizumi TT, Mahesh M. Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology. 2008;248:254–63.
- 9.Fichtner J, Ulrich CT, Fung C, Knüppel C, Veitweber M, Jilch A, et al. Management of spontaneous intracranial hypotension – Transorbital ultrasound as discriminator. J Neurol Neurosurg Psychiatry. 2016;87:650–5.
- 10.Beck J, Fung C, Ulrich CT, Fiechter M, Fichtner J, Mattle HP, et al. Cerebrospinal fluid outflow resistance as a diagnostic marker of spontaneous cerebrospinal fluid leakage. J Neurosurg Spine. 2017;27:227–34.
- 11.Yoshida H, Takai K, Taniguchi M. Leakage detection on CT myelography for targeted epidural blood patch in spontaneous cerebrospinal fluid leaks: calcified or ossified spinal lesions ventral to the thecal sac. J Neurosurg Spine. 2014;21:432–41.
- 12.Allmendinger AM, Lee TC. Spontaneous intracranial hypotension from calcified thoracic disc protrusions causing CSF leak successfully treated with targeted epidural blood patch. Clin Imaging. 2013;37:756–61.
- 13.Rapoport BI, Hartl R, Schwartz TH. Cranial neuropathy due to intradural disc herniation. Neurosurgery. 2014;74:E561–5.
Copyright
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.