Penile horn – successfully treated
Abstract
Glans penis is an unusual site for horn. Only few cases are reported worldwide in English literature. Pseudoepitheliomatous, keratotic, and micaceous balanitis (PKMB) is a pyodermatitis with pseudoepitheliomatous response to chronic inflammation or infection. Rarely it can develop a horn. There is one case report of PKMB presenting as penile horn and one case with nail-like presentation in the literature. Mode of treatment of PKMB with horn ranged from topical 5-fluorouracil, electrosurgery, and cryosurgery to excision. Use of oral acitretin in PKMB or penile horn is unknown. We are reporting a 60-year-old circumcised male who presented with a penile horn. Histology was suggestive of PKMB. Treatment with topical 5-flurouracil did not work. He was successfully treated with oral acitretin.
Keywords: Acitretin, penile horn, pseudoepitheliomatous, keratotic, and micaceous balanitis
Case Report
A 60-year-old circumcised Indian male presented with a gradually enlarging asymptomatic thick, scaly, verrucous plaque on the glans penis for 2 years. He had undergone circumcision for phimosis 8 years ago. There was no history of itching, whitish discoloration of mucosa, or difficulty in urination. Examination revealed a well-defined scaly, verrucous plaque with a hard horn-like projection of 1.75 cm [Figure 1] from surface of the plaque. There was no regional lymphadenopathy. Systemic examination was normal. Based on the morphology, giant condyloma, verrucous carcinoma, PKMB, squamous cell carcinoma, and keratoacanthoma were considered as differentials. Elliptical biopsy from the thick scaly lesion and adjoining normal mucosa from the glans revealed acanthosis, massive hyperkeratosis, pseudoepitheliomatous hyperplasia, and a sparse mononuclear cell infiltrate in the superficial dermis suggestive of PKMB [Figure 2]a, [Figure 2]b, [Figure 2]c. There was no evidence of malignancy or cellular atypia in histopathology. His routine hematological parameters, fasting blood sugar, lipid profile, liver function, and renal function tests were within normal limits. HIV antibody test and venereal disease research laboratory tests were non-reactive. Based on clinical and histopathological features, a final diagnosis of PKMB presenting as penile horn was made and the patient was started on topical 5% 5-fluorouracil. There was no significant improvement after 1 month of treatment. Patient also did not give consent for any surgical methods and cryotherapy. Based on the clinical and histopathological findings of hyperkeratosis and mode of action of acitretin (i.e., normalizing the keratinization and preventing malignancy), we started oral acitretin 25 mg per day. After one and half months of treatment, there was complete disappearance of the horn and 80% improvement of underlying plaque [Figure 3]. The patient did not develop any side effects to acitretin and is currently under follow up.

Figure 1
Verrucous plaque with hard horn-like projection on penis
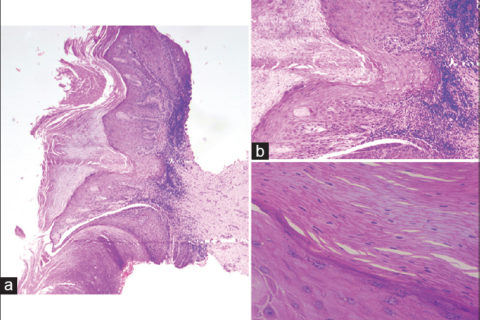
Figure 2: (a) Extensive parakeratosis (H and E ×40).(b) Massive hyperkeratosis, pseudoepitheliomatous hyperplasia, and mononuclear cell infiltrate in superficial dermis (H and E ×100). (c) Acanthosis, parakeratosis, and orthokeratosis (H and E ×400)

Figure 3: Disappearance of horn with marked improvement in plaque following treatment with acitretin
Discussion
“Horn” is a protuberant mass of keratin due to unusual cohesion of keratinized material.[1] Though horn can occur at any site, penis is an unusual site for the same. Till date, <100 cases of penile horn are reported in the world.[2] Penile horns present as elongated, keratinous projections and the etiology is not clear. The various predisposing factors implicated for its development include chronic prepucial inflammation, phimotic foreskin, trauma, poor hygiene, relapsing balanoposthitis, viral infection, and tumor, especially squamous cell carcinoma and verrucous carcinoma.[2],[3] Finding the cause of penile horn is usually made by clinicohistopathological correlation.[10]
PKMB of glans is characterized by hyperkeratotic plaque with an overlying thick micaceous scale. There are <20 cases of PKMB reported in English literature.[11] Majority of reported cases of PKMB had malignant transformation during presentation and hence this entity needs early diagnosis and treatment.[11] Horn-like presentation has been reported by Pai et al.[4] and nail-like presentation reported by Subudhi and Singh et al.[5] PKMB may have locally invasive or aggressive tendencies and should be considered to have low-grade or limited malignant potential.[12] The pathogenesis of PKMB occurs in four stages: (a) initial plaque stage, (b) late tumor stage, (c) verrucous carcinoma, and (d) transformation to squamous cell carcinoma and invasion. Treatment options for PKMB include topical 5-flurouracil, podophyllin resin, and steroids; physical measures like cryotherapy, radiotherapy if underlying pathology is benign, and surgical excision in malignant cases.[13]
Acitretin is a second generation retinoid used in keratinizing disorders. It works by normalizing the keratinization process. It is also used as a chemoprophylactic agent in cutaneous premalignant conditions like actinic keratosis[6],[7] epidermodysplasia verruciformis,[8] graft versus host disease,[14] xeroderma pigmentosa,[9] keratoacanthoma,[15] and basal cell nevus syndrome. Acitretin works by binding with the retinoic acid receptor (RAR gamma receptor specially expressed on adult skin). Thereby it causes expression or suppression of RARE (retinoic acid response element) and m-RNA synthesis, hence causing expression of proteins for induction of differentiation and inhibition of cell proliferation, responsible for anti-tumor effect in premalignant conditions.[16],[17]
Our case presented with asymptomatic penile horn since 2 years. The diagnosis of PKMB with penile horn was made by clinical and histological correlation. The patient had no evidence of any malignant changes in histopathology. Initial treatment with topical 5-fluorouracil did not show appreciable improvement and patient denied cryotherapy or surgery. Hence, oral acitretin 25 mg once a day was started, thinking it would normalize the keratinization process and bring about an improvement. At about one and half months there was disappearance of the horn and 80% improvement of underlying plaque. Previous case report of PKMB presenting as penile horn by Pai et al. did not have a complete cure. Our case is unique for being successfully treated with acitretin 25 mg. Possible mechanism of acitretin in PKMB with penile horn may be due to normalization of epidermal proliferation and induction of differentiation. On reviewing the literature we did not find any report of acitretin use in PKMB or PKMB with horn.
Authors
Chandra Sekhar Sirka1, Kananbala Sahu1, Swetalina Pradhan1, Subhasini Naik2
1 Department of Dermatology, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India
2 Department of Pathology, S.C.B. Medical College, Cuttack, Odisha, India
References
| 1. | Gupta S, Thappa DM, Jaisankar Singh. Giant cutaneous horn. Ind J Dermatol 2000;45:149-50;74:456-7. |
| 2. | Karthikeyan K, Thappa DM, Jaisankar TJ, Balamourougane P. Cutaneous horn of glans penis. Sex Transm Infect 1998;74:456-7. |
| 3. | Thappa DM, Rakesh SV, Karthikeyan K. Penile horn overlying verrucous carcinoma. Indian J Sex Transm Dis 2003;24:33-4. |
| 4. | Pai VV, Hanumanthayya K, Naveen KN, Rao R, Dinesh U. Pseudoepitheliomatous, keratotic and micaceous balanitis presenting as cutaneous horn in an adult male. Indian J Dermatol Venereol Leprol 2010;76:547-9. [PUBMED] [Full text] |
| 5. | Subudhi CL, Singh PC. Pseudoepitheliomatous, keratotic and micaceous balanitis producing nail-like lesion on the glans penis. Indian J Dermatol Venereol Leprol 1999;65:75-7. [Full text] |
| 6. | Belisario JC. Recent advances in topical cytotoxic therapy of skin cancer and pre-cancer. In: Melanoma and Skin Cancer. Proceedings International Cancer Conference, Sydney 1972, p. 349-65. |
| 7. | Bollag W, Ott F. Therapy of actinic keratoses and basal cell carcinomas with local application of vitamin A acid. Cancer Chemotherapy Rep 1971;55:59-60. |
| 8. | Anadolu R, Oskay T, Erdem C, Boyvat A, Terzi E, Gürgey E, et al. Treatment of epidermodysplasia verruciformis with a combination of acitretin and interferon alfa-2a. J Am Acad Dermatol 2001;45:296-9. |
| 9. | Berth-Jones J, Cole J, Lehmann AR, Arlett CF, Graham Brown RA. Xeroderma pigmentosum variant: 5 years of tumour suppression by etretinate. J R Soc Med 1993;86:355-6. |
| 10. | Lowe FC, McCullough AR. Cutaneous horns of the penis: An approach to management. Case report and review of the literature. J Am Acad Dermatol 1985;13:369-73. |
| 11. | Schellhammer PF, Jordan GH, Robey EL, Spaulding JT. Premalignant lesions and nonsquamous malignancy of the penis and carcinoma of the scrotum. Urol Clin North Am 1992;19:131-42. |
| 12. | Reed SI, Abell E. Pseudoepitheliomatous, keratotic and micaceous balanitis. Arch Dermatol 1981;117:435-7. |
| 13. | Perry D, Lynch PJ, Fazel N. Pseudoepitheliomatous, keratotic, and micaceous balanitis: Case report and review of the literature. Dermatol Nurs 2008;20:117-20. |
| 14. | Borroni RG, Poddighe D, Zecca M, Brazelli V. Efficacy of acitretin for porokeratosis in a child with chronic cutaneous graft versus host disease. Paediatr Dermatol 2013;30:148-50. |
| 15. | Robertson SJ, Bashir SJ, Pichert G, Robson A, Whittaker S. Severe exacerbation of multiple self-healing squamous epithelioma (Ferguson-Smith disease) with radiotherapy, which was successfully treated with acitretin. Clin Exp Dermatol 2010;35:e100-2. |
| 16. | Breitman TR, Selonick SE, Collins SJ. Induction of differentiation of the human promyelocytic leukemia cell lines (HL-60) by retinoic acid. Proc Natl Acad Sci USA 1980;77:2936-40. |
| 17. | Lotan R. Effects of vitamin A and its analogs (retinoids) on normal and neoplastic cells. Biochim Biophys Acta 1980;605:33-91. |