Skull Repair after Major Crush Injury
H. Sudhoff, 1 ,* H. J. Hoff, 2 and M. Lehmann 1
Case Report
A 48-year-old German safety officer suffered compression injury to his cranial vault whilst examining a pressing machine (Figure 1(a)). The accidental onset of the machine resulted in severe compression of his skull. This led to compound comminuted skull and facial fractures (parietal, sphenoid, frontal, orbital rim, ethmoid, maxillary, zygomatic, and nasal bones) (Figure 1(b)). This trauma left him with right-sided hemiplegia, right-sided total blindness, and loss of bony covering on the left side of his brain. Six months after primary trauma surgery, he presented to the ENT department for definitive reconstruction of the skull and right-sided dacryocystorhinostomy to treat his right-sided epiphora.

Figure 1.
(a) Shows on the left an obvious skull deformity after crush injury. Bone is largely missing and the left orbital margin is severely compromised. The right eye is removed. (b) A composite 3D reconstruction of the patient’s skull showing the extensive bone loss and sequelae of multiple skull and facial fractures.
A computer-assisted designed/computer-assisted modeled (CAD/CAM) titanium implant for cranioplasty was manufactured using the DICOM high-resolution CT dataset (Figure 2). The patient underwent bilateral cranial tissue expander insertion 8 weeks prior to reconstructive surgery. Three months prior to reconstruction, a skin expander was implanted to ensure a tension-free closure of the defect.

This figure shows a computerized reconstruction of the bony defect. This is used as a template for construction of a titanium cranioplasty prosthesis.
After dissection of the overlying scared skin, the dura was exposed. The titanium cranioplasty prosthesis installed and fixed with self-drilling 7 mm screws (Figure 3). The fit was excellent. The previous tissue expansion resulted in tension-free skin closure over the implant (Figure 4(a)). Drains were placed for the initial 48 hours. Excess skin was left in expectation of flattening as healing occurred (Figure 4(b)). This was found to be the case at 1 week after surgery (Figure 5). The placeholder positioned during right-sided dacryocystorhinostomy was removed 3 months prior to the initial surgery.

Prereconstruction photograph. Due to the expected skin loss, two inflatable skin expanders had been inserted.

Figure 4
(a) Shows the “in situ” titanium cranioplasty. Note the fit and screw fixation to the defect margins. (b) Postoperative view after tension-free skin closure.
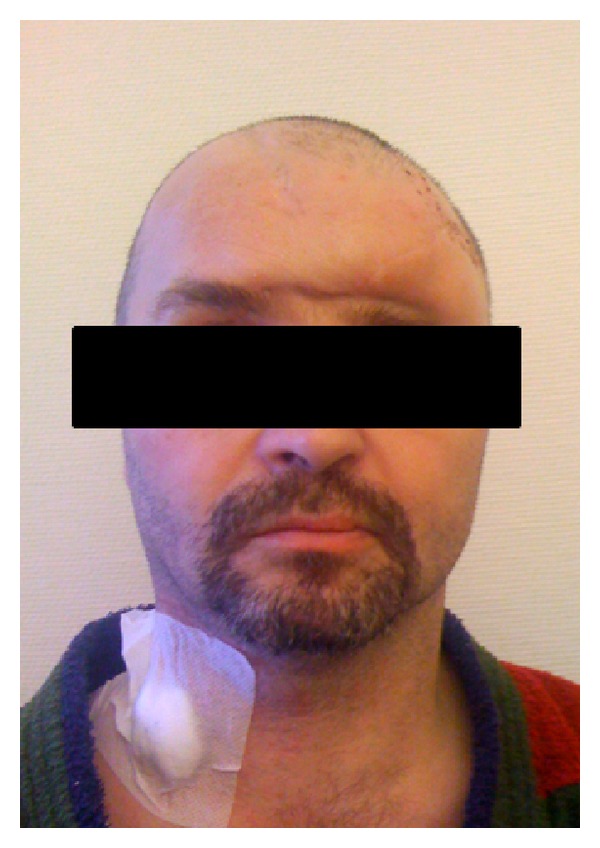
Figure 5
Showing the patient one week after surgery. The missing bone has been replaced by the titanium cranioplasty prosthesis. Wound healing was excellent and the excess skin flattened. A prosthesis will be fitted to replace his right eye.