Thoracic Stab Wound: A Curious Case Report
Case Presentation
A 38-year-old male, a chronic alcoholic who committed an attempt of suicide, was presented to the emergency department of the University Hospital “St. George”- Plovdiv. On initial presentation, the patient was in a prone position, awake, oriented, and hemodynamically stable (blood pressure 140/90 mmHg and heart rate 92 bpm). The external examination revealed no clothing on the chest with entirely impaled knife (just to its handle) in the left hemithorax, approximately 5 cm medially to the left nipple (Figure 1).

Figure 1: Impaled knife in the left hemithorax, approximately 5 cm medially to the left nipple.
Physical examination established respiratory rate 18 breaths per minute and slightly diminished left breath sounds.
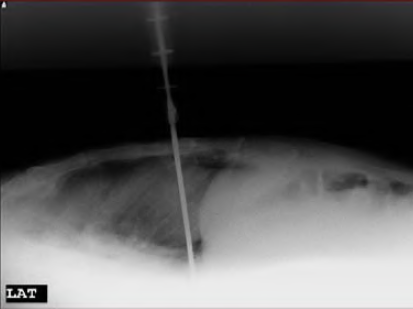
Lateral chest radiograph in a prone position of the patient demonstrated a knife, penetrating int the left hemithorax (Figure 2). No evidences of pneumothorax and hemothorax and no widening of the cardiac silhouette were established.
is demonstrated.

Figure 3: A knife passed through the oblique fissure of the left lung is
presented.
The patient was transferred from emergency department to the operating room of the
Department of Thoraco-Abdominal Surgery and left lateral thoracotomy was performed
immediately. Exploration of the thoracic cage established that the knife had passed through the oblique fissure of the left lung, causing a small linear laceration of outer surface of the lingula (Figure 3). The point of the knife was in a contact with the pericardium of the left ventricle without pericardial penetration. Approximately 100 ml of blood were aspirated from the left costophrenic sulcus. The knife (blade with length 20 cm an maximal width 25 mm) was removed (Figure 4). The minor lung laceration was over sewed and the chest wall knife’s tract was sutured.
The patient was discharged at the 7th day after his admission,
without postoperative complications and without any pathology on
control chest radiograph.
