A bullet lodged in the neck
Case Report:
A 27-year-old African-Ugandan woman of Nilotic ethnicity presented to the Accident and Emergency Department of a tertiary hospital, following a GSI to her face. The injury was the result of a ‘stray’ bullet, shot from an AK-47 submachine gun at a distance of about 70m. Resuscitation and a surgical wound toilet were done without extension of the wound. Essential antibiotics and vaccines were administered, and the wound was dressed (not sutured). Injuries had been sustained over the right side of her face, leaving a large open wound.
She was referred to the tertiary hospital 10 days after these events. Her main complaints were right mandibular pain, with difficulty in opening her mouth and chewing, and inability to hear with her right ear. There was a laceration of her maxillomandibular area (6cm in length) with features of infected granulation tissue (Figure 1). The right side of her maxillofacial region was swollen and tender. There was no active bleeding, subcutaneous emphysema, or dyspnea and stridor. She had only a very limited capacity to open her jaw, and even then with pain. There was no particularly painful area in her neck. Remarkable findings were revealed on cranial nerve examination. She had a right facial nerve palsy (lower motor neuron) and total loss of cutaneous sensation over the distribution of the right maxillary and mandibular branches of her trigeminal nerve in the maxillary and mandibular regions respectively. The ophthalmic division of her trigeminal nerve was intact. Her auditory function was assessed.

Figure 1
Appearance of the wound 10 days after injury. There is evidence of suppuration and areas of granulation tissue formation.
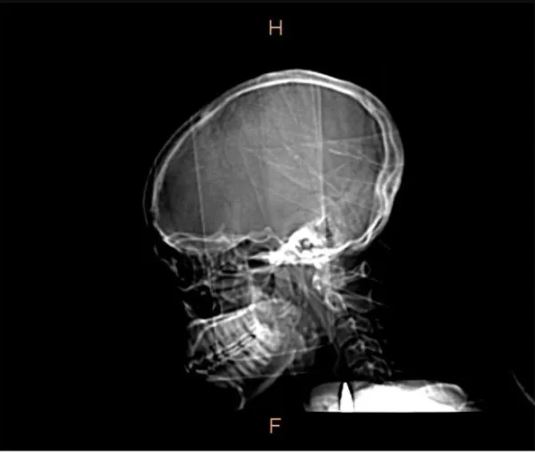
A plain radiograph of her head and neck (Figures 2 and 3) and an ultrasound scan of her neck, done prior to her referral, had revealed the presence of a bullet in the right side of her neck, anterior to cervical vertebrae 6 and 7. Basic as it is, this plain radiograph enabled identification of this important condition.
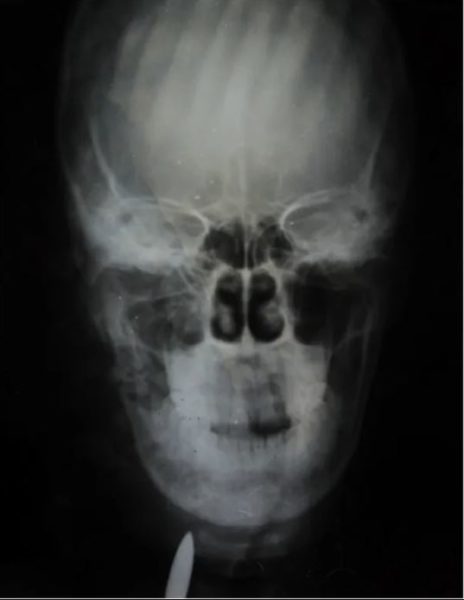
This shows a bullet in the right side of the neck. Comminuted fracture of the mandible (angle and ramus) and maxillary antrum are revealed.

This shows a bullet lodged in the neck, anterior to the bodies of cervical vertebrae 6 and 7.
A comminuted fracture of the ramus and angle of her right mandible was confirmed. Further evaluation involved conducting a CT scan of her head and neck 1 week after admission. This confirmed the earlier radiological findings; a bullet not only lodged in the right side of her neck but within her carotid sheath as well (Figure 4). The CT scan however, showed that it was no longer positioned just anterior to cervical vertebrae 6 and 7, but also anterior to cervical vertebra 5.
The scan shows a cephalad shift of the bullet to lie partially anterior to the fifth cervical vertebra. There is also a comminuted fracture of the angle and ramus of the right mandible. The section is through the median sagittal plane.
A right longitudinal cervical incision, just posterior and parallel to her sternocleidomastoid muscle, was used to access the posterior triangle of her neck. The investing deep fascia was dissected and her carotid sheath opened. The bullet was identified, confined within a pocket of debris (Figure 5). There were no signs of suppuration, and acute inflammation had resolved. The debris possibly consisted of damaged tissue encountered along the trajectory of the bullet: parotid gland tissue, blood, nerve and muscle remnants. The bullet was extracted, debris was flushed out thoroughly with normal saline and her sheath was closed with Vicryl 2–0 continuous suture (Figure 6).

Figure 5

Figure 6
Credits: Peter A Ongom