Diagnosis and management of a giant ovarian cyst in the gravid-puerperium period: a case report
Sibraogo Kiemtoré,1,2Hyacinthe Zamané,1,2Yobi Alexis Sawadogo,1Rodrigue Sansan Sib,3Evelyne Komboigo,2Ali Ouédraogo,1 and Blandine Bonané1,2
Sociodemographic characteristics of the patient
The patient was a 25-year-old woman who dropped school early and got married with a single farmer. She lived with her husband in Kongoussi, a rural commune about 100 km from Ouagadougou, the capital city of Burkina Faso. She did not have any income-generating activity. She had her first menses at 16 years old. She was third gravida and third para with three living children.
Diagnostic approach
For her previous pregnancy, the date of the patient’s last menses was not known and no dating ultrasound was performed. She received prenatal care at the health center of her village, but no paraclinic investigation was carried out during her pregnancy.
On November 18th, 2018, the patient gave birth to a baby boy at health center of her village. At birth, the baby had Apgar’s score of 8/10 at the first minute, 10/10 at the 5th minute, and weighed 2780 g. The patient reported that after her last delivery her abdomen had remained large as compared to previous deliveries. She also said to have noticed a gradual increase in the volume of her abdomen in the days following delivery. As she unsuccessfully went through traditional care made of decoction, 10 days after giving birth, she decided to go back to the health center of her village for consultation. From this center, she was referred to the Department of Obstetrics Gynecology at Yalgado Ouedraogo University Hospital Center in Ouagadougou, 27 days after giving birth, i.e. on December 15, 2018. At admission, she was complaining of tension-type abdominal pain and was dyspnetic. She weighed 93 kg and was 167 cm tall with a temperature of 37°2 C. On inspection, the abdomen was largely distended (Fig. 1). As for the palpation, it revealed an enormous abdominopelvic mass with a dull note on percussion. The abdominal perimeter was 126 cm long.

Abdominal distension before removal of abdominal cyst
An ultrasound found a cystic abdominopelvic image without being able to attach it to an organ. It was then that a Computed tomography (CT) was performed. This CT also showed a fluid mass with no evidence of solid components or septations (Fig. 2). In this regard, the radiologist discussed two diagnoses: a giant ovarian cyst and a huge mesenteric cyst. The tumor marker CA-125 was normal and the haemoglobin blood level was 14.5 g per deciliter.
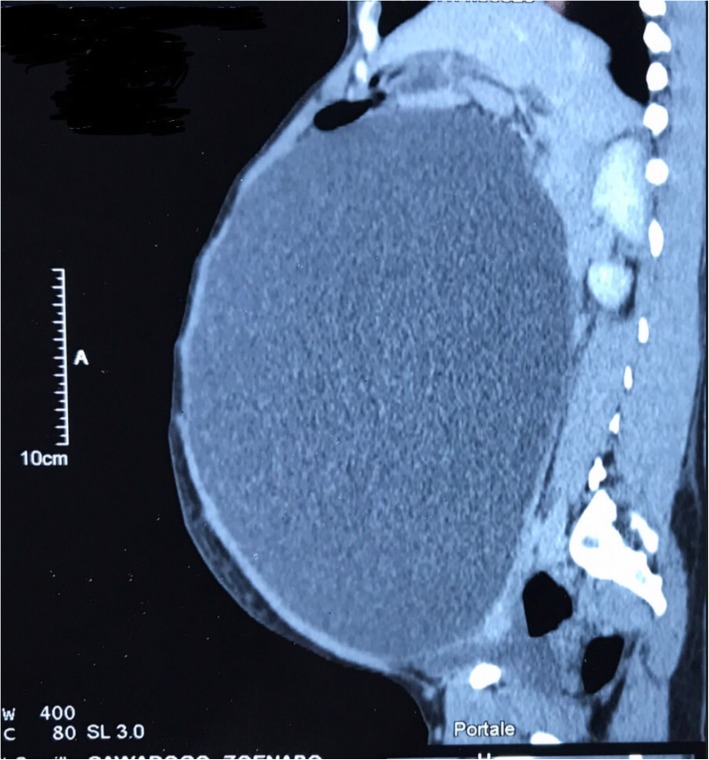
abdominopelvic unilocular cyst by CT scan
Treatment
We performed a midline laparotomy from the lower abdomen up to the umbilicus (Fig .3) that allowed the externalization of the cyst located in the left ovary (Fig. 4). The uterus and contralateral adnexa were macroscopically normal. We then carried out a left total oophorectomy. The removal of the latter giant ovarian cyst allowed an exploration of the entire abdominal cavity. But we did not find any ascites or abnormalities of the other intraperitoneal organs (Fig. 5). The abdominal wall was closed by some simple interrupted sutures. The fascia was closed with decimal 4 polyglactin sutures and the skin with decimal 3 non-absorbable sutures. The patient’s abdomen turned flat immediately after surgery (Fig. 6). The removed cyst measured 42 cm long-axis and weighed 19.7 kg (Fig. 7). The postoperative period was uneventful and the patient was released from the hospital on the 3rd day after surgery. No complications were observed in the 45 days after surgery. At the histological study, the cyst was benign and was viewed as a serous ovarian cystadenoma.

Fig. 3
incision from in the lower abdomen up to the umbilicus

Fig. 4
externalization of the giant cyst

Fig. 5
exploration of the entire abdominal cavity; no ascites, no abnormalities of the other intraperitoneal organs found

abdomen turned flat immediately after surgery

Fig. 7
giant ovarian cyst after removal (19,7 kg and 42 in cm in diameter)
Author information
1Training and Research Unit in Health Sciences, University Joseph Ki-Zerbo, 7021, Ouagadougou 03, BP Burkina Faso
2Yalgado Ouedraogo teaching hospital, 7022, Ouagadougou 03, BP Burkina Faso
3School of Health Sciences, Polytechnic University of Ouahigouya, Ouagadougou 03, BP 36 Burkina Faso
Sibraogo Kiemtoré,
Copyright and license information
Copyright © The Author(s). 2019Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
References
References
- Schwartz N, Timor-tritsch IE, Wang E. Adnexal masses in pregnancy. Clin Obstet Gynecol. 2009;52(4):570–585. doi: 10.1097/GRF.0b013e3181bea9d7. [PubMed] [CrossRef] [Google Scholar]
- Agah J, Jafarzadeh Esfehani R, Kamalimanesh B, Fattahi Abdizadeh M, Jalilian AR. Mismanagement of a huge ovarian serous cystadenoma in a young girl; a case report. J midwifery Reprod Heal. 2015;3(1):315–317. [Google Scholar]
- De Lima SHM, dos Santos VM, Daros AC, Campos VP, Modesto FRD. A 57-year-old Brazilian woman with a giant mucinous cystadenocarcinoma of the ovary: a case report. J Med Case Rep. 2014;4:82. doi: 10.1186/1752-1947-8-82. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Bhasin S k, Kumar V, Kumar R. Giant ovarian cyst: a case report. JK Sci. 2014;16:3.
- Schemeler K, Mayo-Smith WW, Reipert JF, Weitzen S, Manue IMD, Gordinier ME. Adnexal masses in pregnancy: surgery compared with observation. Obstet Gynecol. 2005;105:1098. doi: 10.1097/01.AOG.0000157465.99639.e5. [PubMed] [CrossRef] [Google Scholar]
- Hota BM, Rukmini KR, Basavaih PGC. Giant ovarian cyst in term pregnancy – a rare case report. Bali Med J. 2015;4(1):5–7. [Google Scholar]
- Nemec U, Nemec SF, Bettelheim D, Brugger PC, Horcher E, Schöpf V, et al. Ovarian cysts on prenatal MRI. Eur J Radiol. 2012;81(8):1937–1944. doi: 10.1016/j.ejrad.2011.04.047. [PubMed] [CrossRef] [Google Scholar]
- Mukhopadhyay A, Shinde A, Naik R. Ovarian cysts and cancer in pregnancy. Best Pract Res Clin Obstet Gynaecol. 2016;33:58–72. doi: 10.1016/j.bpobgyn.2015.10.015. [PubMed] [CrossRef] [Google Scholar]
- Naqvi M, Kaimal A. Adnexal masses in pregnancy. Clin Obstet Gynecol. 2015;58(3):93–101. doi: 10.1097/GRF.0000000000000088. [PubMed] [CrossRef] [Google Scholar]
- Casarotto A, Cerofolini A, Denitto F. Mesenteric cyst: case report and review of the literature. G Chir. 2010;31:239e242. [PubMed] [Google Scholar]
- Rossato M, Burei M, Vettor R. Giant mucinous cystadenoma of the ovary mimicking ascites: a case report. Clin Med Rev Case Rep. 2016;3:103. doi: 10.23937/2378-3656/1410103. [CrossRef] [Google Scholar]
- Elhassan M, S A Khan S, El-Makki A. Giant ovarian cyst masquerading as massive ascites in an 11-year-old. Case Rep Pediatr. 2015;4:5. [PMC free article] [PubMed] [Google Scholar]
- Kassidi F, Moukit M. Ait El Fadel F, El Hassani M, Guelzim K, Babahabib a, et al. successful management of a giant ovarian cyst: a case report. Austin Gynecol Case Rep. 2017;2:1012–1016. [Google Scholar]
- Yeika EV, Efie DT, Tolefac PN, Fomengia JN. Giant ovarian cyst masquerading as a massive ascistes: a case report. BMC Res Notes. 2017;10:749. doi: 10.1186/s13104-017-3093-8. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Casanelli JM, Keita M, N’Dri AG, Moussa B, Blegole C, et al. Kyste géant de l’ovaire en Côte d’ivoire. Med Sante Trop. 2010;70:122. [PubMed] [Google Scholar]
- Qublan H, Al-Ghoweri A, Al-Kaisi N, Abu-Khait S. Benign mucinous cystadenoma with stromal luteinization during pregnancy: a hormonally responsive tumor and a rare cause of fetal intrauterine growth restriction. J Obs Res. 2002;28:104–107. [PubMed] [Google Scholar]
- Petros M, Koliba P, Sevcík L, Curík R. Giant benign mucinous cystadenoma of both ovaries in early puerperium: case report and review of literature. Cesk Gynekol. 2005;70(2):156–158. [PubMed] [Google Scholar]
- Noreen H, Syed S, Chaudhri R, Kahloon L. A large unilocular mucinous cystadenoma in third trimester of pregnancy. J Coll Physicians Surg Pak. 2011;21:426–428. [PubMed] [Google Scholar]
- Baradwan S, Sendy F, Sendy S. Giant ovarian cyst in pregnant woman had uncomplicated term vaginal delivery and treated laparoscopically postpartum : a case report. Merit Res J Med Med Sci. 2017;5(8):366–369. [Google Scholar]
- Rosales AE. Giant ovarian cyst and pregnancy. Case report and literature review. Ginecol Obstet Mex. 2011;79:235–238. [PubMed] [Google Scholar]
- Cheng EJ, Kurman RJ, Wang M, Oldt R, Wang BG, Berman DM, et al. Molecular genetic analysis of ovarian serous cystadenomas. Lab Investig. 2004;84(6):778–784. doi: 10.1038/labinvest.3700103. [PubMed] [CrossRef] [Google Scholar]
Articles from BMC Pregnancy and Childbirth are provided here courtesy of BioMed Central
Original source
Changes from original article
Sensitive parts have been censored, in contrast from the original source where they are not censored.