Eye Inside Out After Getting Hit By a Bull Horn
Girish S. Mishra, MS1 and Sushen Harish Bhatt, MS1
Case History
A 68-year-old female, member of low socioeconomic community, presented to the casualty with history of hit over the right eye by a bull horn during her daily agricultural activities. She complained of sudden and painful loss of vision in the right eye. She also had a history of minimal amount of right nose bleed which was spontaneously controlled without any intervention. No other significant injuries were noted. She had no known comorbidities.
Clinical Findings
Patient was vitally stable with a good general condition. Ophthalmological examination revealed an empty right eye socket with both upper and lower lid edema (Fig. 1). The right eye could not be located. An unreliable perception of light was marked in the same eye. A palpable fracture of the inferior orbital rim was noted. Nose examination revealed blood clots in the right nostril. Other examinations seemed normal.

Fig. 1
Presenting image of patient where the right orbital socket is empty.
Diagnostic Assessment
Ultrasonographic B scan was done which revealed the right eye to be displaced posteroinferomedially with restricted movements but a normal lens in situ. Computed tomography scan was done which showed orbital blow-out fracture involving the medial wall and floor, with the right eye lying in the right anterior ethmoid cells going into the anterior part of the right nasal cavity (Figs. 2 and 3). Fortunately, the respective optic nerve was seen in contact and was in continuity with the displaced eyeball and it seemed to be intact.

Coronal CT scan of the orbit showing posteroinferomedial displacement of the right eyeball into the nasal cavity

Axial CT scan of the orbit showing posteroinferomedial displacement of the right eyeball into the nasal cavity.
Therapeutic Intervention
Hence interventional surgery was planned under general anesthesia. Nasal endoscopy showed a globular bulge on the lateral wall of the nose displacing the uncinate process, middle turbinate and fractured pieces of ethmoids medially. Uncinectomy was done and fractured lamina papyracea was observed. The soft-tissue bulge caused by the eyeball was pushed laterally and anteriorly back into its socket with utmost care and precision using a Freer elevator. Simultaneously, our ophthalmology colleagues took a loop suture over the lateral rectus and pulled the eye in its position (Fig. 4). Lose fragments of fractured ethmoids were removed. The septal cartilage was harvested by giving a Freer incision. The cartilage was then kept over the defect on the lateral wall as a support. The size of the septal cartilage was approximately 2 × 2 cm. The cartilage was encased within a Surgicel and was kept over the lateral nasal wall defect by insinuating between the fractured edges of lamina papyracea between the orbital fat and lamina papyracea and it was supported by merocele anterior nasal pack.
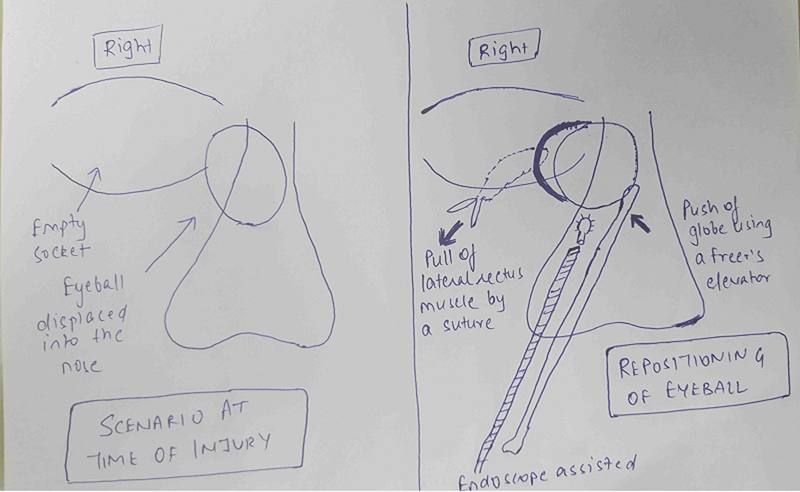
Schematic image of the operative intervention by pushing the globe laterally using the Freer elevator and pulling it by the loop suture attached to the lateral rectus muscle.
On table findings revealed an intact globe with a clear healthy cornea. Multiple conjunctival tears with muscle lacerations were seen (Fig. 5). Pupil was 3 mm dilated, not reactive to light, and there was immature cataract.
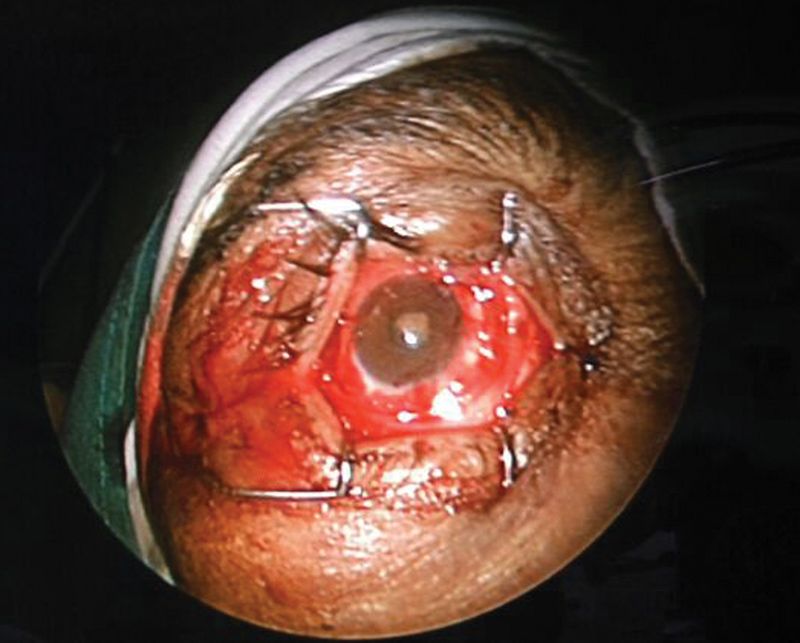
On table findings of the right eye after successful reposition of the globe.
Follow-Up and Outcome
On the first postoperative day, the woman gained a visual acuity of counting fingers at 1.5 m for distance and N18 (Faculty’s Roman test types notation) or J10 (Jaeger notation) for near in the operated right eye. Postoperative edema was present with congestion and chemosis. There was mechanical ptosis with restricted movements and exotropia. There was no diplopia. Slit-lamp examination showed a clear cornea, quiet anterior chamber, and a 3-mm diameter pupil sluggishly reactive to light. Intraocular pressure was normal (12 mm Hg). Finally, fundus examination showed a normal optic disc and macula.
Subsequent follow-ups showed an improvement in visual acuity achieving 6/24 (Snellen’s visual acuity) or –0.6 (log equity relative to 20/20) or 4.0 (minimal angle of resolution [MAR]) vision in distance and N18 (Faculty’s Roman test types notation) or J10 (Jaeger notation) in near. Ptosis also improved. Pupil became fully reactive to light. Mild exotropia with restriction of movements, however, persisted.
The latest follow-up done at 8 months has showed a visual acuity of 6/18 (Snellen’s visual acuity) or –0.5 (Log equity relative to 20/20) or 3.0 (MAR) for distance and N18 (Faculty’s Roman test types notation) or J10 (Jaeger notation) for near. There is minimal restricted movement. And on the latest follow-up, there is no ptosis at all. With mild restriction in left lateral gaze, there is occasional diplopia on lateral gaze of the opposite side due to compression of the medial rectus at the time of the injury. However, the patient does not find it much troublesome and her daily routine life is not affected (Fig. 6). Follow-up CT scan also shows a normally placed globe (Figs. 7 and 8).

Patient’s condition at 8 months postoperative period.
Conclusion
Early surgical intervention is the key to good visual outcome in orbital blowout fractures. Endonasal endoscopic approach to medial orbital blow out fractures gives a promising result and must be promoted due to multilevel benefits. Preoperative evaluation of retina and optic nerve gives a clue on the likely visual prognosis. Thus, we recommend that every patient of displaced eye deserves a surgical intervention.
Author Information
1Department of Otorhinolaryngology, Head and Neck Surgery, Pramukh Swami Medical College and Shri Krishna Hospital, Anand, Gujarat, IndiaAddress for correspondence Sushen Harish Bhatt, MS Department of Otorhinolaryngology, Head and Neck Surgery, Pramukh Swami Medical College and Shri Krishna Hospital, Karamsad Anand Gujarat 388325, India,
References
1. Ko M J, Morris C K, Kim J W, Lad S P, Arrigo R T, Lad E M. Orbital fractures: national inpatient trends and complications. Ophthal Plast Reconstr Surg. 2013;29(4):298–303. [PubMed] [Google Scholar]2. Vats S, Murthy G V, Chandra M, Gupta S K, Vashist P, Gogoi M. Epidemiological study of ocular trauma in an urban slum population in Delhi, India. Indian J Ophthalmol. 2008;56(4):313–316. [PMC free article] [PubMed] [Google Scholar]3. Nirmalan P K, Katz J, Tielsch J M. et al.Ocular trauma in a rural south Indian population: the Aravind Comprehensive Eye Survey. Ophthalmology. 2004;111(9):1778–1781. [PubMed] [Google Scholar]4. Burm J S, Chung C H, Oh S J. Pure orbital blowout fracture: new concepts and importance of medial orbital blowout fracture. Plast Reconstr Surg. 1999;103(7):1839–1849. [PubMed] [Google Scholar]5. Motamedi M H, Dadgar E, Ebrahimi A, Shirani G, Haghighat A, Jamalpour M R. Pattern of maxillofacial fractures: a 5-year analysis of 8,818 patients. J Trauma Acute Care Surg. 2014;77(4):630–634. [PubMed] [Google Scholar]6. Boffano P, Roccia F, Gallesio C, Karagozoglu K H, Forouzanfar T. Diplopia and orbital wall fractures. J Craniofac Surg. 2014;25(2):e183–e185. [PubMed] [Google Scholar]7. Yab K, Tajima S, Ohba S. Displacements of eyeball in orbital blowout fractures. Plast Reconstr Surg. 1997;100(6):1409–1417. [PubMed] [Google Scholar]8. Converse J M, Smith B, Obear M F, Wood-Smith D. Orbital blowout fractures: a ten-year survey. Plast Reconstr Surg. 1967;39(1):20–36. [PubMed] [Google Scholar]9. Singh R I, Thomas R, Alexander T A. An unusual case of bull gore injury. Aust N Z J Ophthalmol. 1986;14(4):377–379. [PubMed] [Google Scholar]10. Miabi Z, Nezami N, Midia M, Midia R. Intracranial displacement of the eye after blunt trauma. J Neuroophthalmol. 2009;29(4):311. [PubMed] [Google Scholar]11. Gollapudi P R, Nandigama P K, Maila S K, Karla R, Kotakadira S. Traumatic intracranial prolapse of eye ball – a case report. Br J Neurosurg. 2013;27(1):114–116. [PubMed] [Google Scholar]12. Kang B D, Jang M H. A case of blowout fracture of the orbital wall with eyeball entrapped within the ethmoid sinus. Korean J Ophthalmol. 2003;17(2):149–153. [PubMed] [Google Scholar]13. Jin H R, Shin S O, Choo M J, Choi Y S. Endonasal endoscopic reduction of blowout fractures of the medial orbital wall. J Oral Maxillofac Surg. 2000;58(8):847–851. [PubMed] [Google Scholar]14. Wu W, Yan W, Cannon P S, Jiang A C. Endoscopic transethmoidal and transconjunctival inferior fornix approaches for repairing the combined medial wall and orbital floor blowout fractures. J Craniofac Surg. 2011;22(2):537–542. [PubMed] [Google Scholar]15. Shi W, Jia R, Li Z, He D, Fan X. Combination of transorbital and endoscopic transnasal approaches to repair orbital medial wall and floor fractures. J Craniofac Surg. 2012;23(1):71–74. [PubMed] [Google Scholar]16. Jeon S Y, Kwon J H, Kim J P. et al.Endoscopic intranasal reduction of the orbit in isolated blowout fractures. Acta Otolaryngol Suppl. 2007;(558):102–109. [PubMed] [Google Scholar]17. Rhee J S, Chen C T. Endoscopic approach to medial orbital wall fractures. Facial Plast Surg Clin North Am. 2006;14(1):17–23. [PubMed] [Google Scholar]18. Humphrey C D, Kriet J D. Surgical approaches to the orbit. Oper Tech Otolaryngol–Head Neck Surg. 2008;19(2):132–139. [Google Scholar]19. Goldblum D, Frueh B E, Koerner F. Eye injuries caused by cow horns. Retina. 1999;19(4):314–317. [PubMed] [Google Scholar]20. Onyekwe L O, Ohaegbulam S C. Penetrating orbito-cranial and ocular cow-horn injuries. Niger J Clin Pract. 2007;10(2):177–179. [PubMed] [Google Scholar]21. Ibrahim O, Olusanya B. Occupational cow horn eye injuries in Ibadan, Nigeria. Ann Med Health Sci Res. 2014;4(6):959–961. [PMC free article] [PubMed] [Google Scholar]
Articles from Craniomaxillofacial Trauma & Reconstruction are provided here courtesy of SAGE Publications
Copyright and License Information
Copyright © Thieme Medical Publishers