Hemicorporectomy: A Case Report
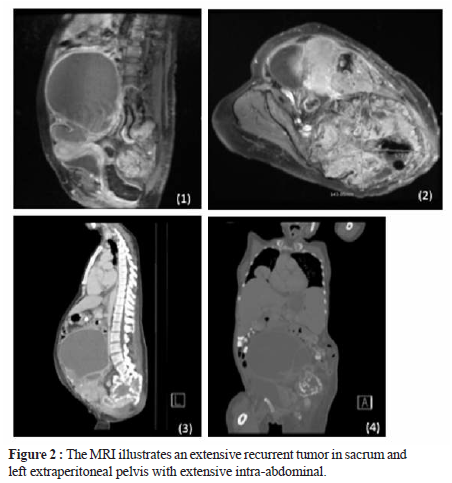
In this case we have a 51-year-old female with recurrent giant cell tumor at left proximal femur with lung metastasis. She was previously diagnosed with giant cell tumor at left sacrum and ilium once, then underwent internal hemipelvectomy in 2009, but the disease recurred. She came to the hospital with progressive peritonitis. The MRI in June, 2017 showed an extensive recurrent tumor in sacrum and left extraperitoneal pelvis.
Indications for surgery in this patient were:
- Acute peritonitis with uncontrolled infection.
- Inadequate soft tissue coverage after simple external
hemipelvectomy. - Benign bone tumor with chance of long term survival.
Operation procedures
On March, 2017, hemicorporectomy at level of L5-S1 was performed with agreement and consent of patient and her family. Multidisciplinary team including colorectal, urologic, vascular surgeons, ICU care team, endocrinologist, psychiatrists, and rehabilitation co-operated to prepare steps of operation and post-operative care. Patient was laid in supine position. The operation started with ligation of IVC and bilateral internal iliac a. Ureterostomy and colostomy was done respectively. Abdomen was temporarily closed for further operations.

After the patient was infection-free and pain was tolerated, rehabilitation was the next step in this patient. Upper-limb strength-training exercises are required to provide adequate power for transfer and locomotion. Sitting upright started in a semirecumbent position then sequentially increased the position. Active range of motion exercise of upper extremities, breathing exercise with incentive breathing spirometer (Triflow) and muscle strengthening exercises were provided as tolerated. Seat cushion from cut-out foam was also applied instead of using total contact orthosis. With aid from the rehabilitation department, a translumbar socket was applied on 31 July 2017. No pressure sore was detected. The translumbar socket allowed her to move from supine to sit and transfer to wheelchair independently. The socket was designed to have ‘mail slots’ for the colostomy and ureterostomy, shown in Figure 5. The platform was also platform-extended to increase the stability. The socket was tailor-made. There was also an addition of a rocker bottom at the distal platform to allow smoother forward progression by using arms for a swing-through gait.
She can now change her own ureterostomy and colostomy by herself with a little assistance of her caregiver. She is independent of her self-care and was trained in basic wheelchair skills. She developed a fair sitting balance.

socket, this patient developed a fair sitting balance.
Conclusion
Hemicorporectomy is an operation of disarticulation of pelvis and lower extremities. It is an undeniably a major operation, but not a harmful one. With a well-organized multidisciplinary team and good comprehension of operation steps, hemicorporectomy can be performed safely as a life-saving operation.