STEMI Associated with Overuse of Energy Drinks
2. Case Presentation
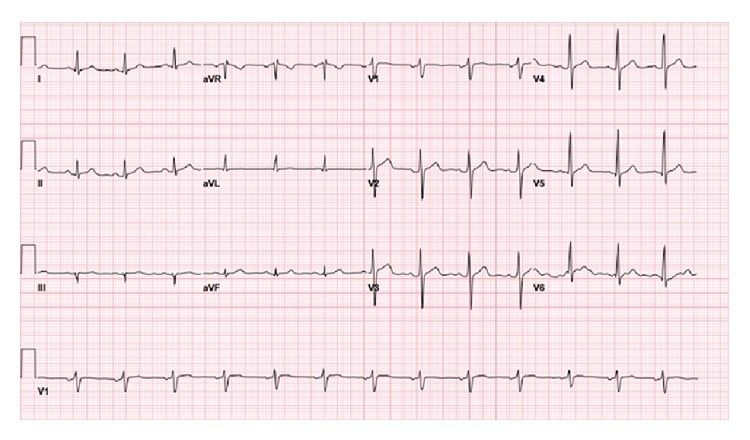
The patient was a 26-year-old male who began having left-sided chest pain approximately 9 hours prior to presentation to the emergency department following drinking his usual quantity (~4L) of “Monster,” “Rock Star,” and other similar brands of energy drinks. The patient stated that he drank any kind of energy drink he could get access to: approximately eight to ten 473 mL drinks per day. The chest pain radiated to his left arm and his jaw but did not worsen with exertion. He also complained of numbness to his left arm, diaphoresis, nausea, and vomiting. His vital signs included a heart rate of 69, blood pressure of 132/73 mm/Hg, respiratory rate of 12, and oxygen saturation of 95% on room air. The patient was in significant distress and was diaphoretic, though not actively vomiting. The patient’s heart showed regular rate and rhythm, lungs were clear to auscultation with no crackles, wheezes, or rhonchi, and the abdomen was soft and nontender without guarding or rigidity. His EKG showed significant ST-elevation in the inferior leads with reciprocal changes in the anterior leads (Figure 1). His initial troponin was 0.02 μg/L (range 0–0.08 μg/L) and CK-MB was 160.1 μmol/L (range 0–266.9 μmol/L); both tests were performed on a point-of-care testing device. The patient was taken to the cardiac catheterization lab before serial blood tests or further formal lab tests could be performed. The patient’s serum caffeine concentration was not obtained, and the energy drink usage did not become known until after the patient had returned from the catheterization. The patient denied any illicit drug or stimulant use, and his urine toxicology screen was negative for any illicit drugs or stimulants, including common benzodiazepines, opiates, δ-9-tetrahydrocannabinol, amphetamines, and cocaine. The patient did however admit to smoking for the last two years, with approximately one pack (20 cigarettes) per day. The results of the patient’s lipid profile were as follows: total cholesterol 5.65 μmol/L (range 1.30–5.18 μmol/L), HDL 0.96 (range 1.04–1.53 μmol/L), LDL 2.69 μmol/L (range <2.59 μmol/L), and triglycerides 4.36 μmol/L (range 0.40–1.70 μmol/L). The patient had no history of diabetes, and each blood sugar check during his hospitalization was less than 6.11 μmol/L (range 3.86–5.55 μmol/L), but HbA1C was not checked. The patient’s complete blood count and complete metabolic panel were within normal limits.

Initial electrocardiogram, showing evidence of acute inferior myocardial infarction.
The patient underwent cardiac catheterization where a 100% occlusion of the left circumflex artery was observed, so a drug-eluting stent was placed after balloon angioplasty. The catheterization report is silent on the presence of any underlying coronary artery plaque in this region. The patient had “mild irregularities” in his left anterior descending coronary artery, in addition to the left circumflex artery occlusion, but no other coronary artery disease in his other coronary vessels was noted. His ST-elevation completely resolved after the catheterization (Figure 2). He remained in the hospital for two days after stent placement and experienced no further chest pain. He was discharged with prescriptions for an antiplatelet agent, an ACE inhibitor, a beta blocker, and a statin, and he agreed to stop smoking and consuming energy drinks.
Electrocardiogram following cardiac catheterization and balloon angioplasty, showing resolution of inferior ST-elevation.
References
- Ali F., Rehman H., Babayan Z., Stapleton D., Joshi D. D. Energy drinks and their adverse health effects: a systematic review of the current evidence. Postgraduate Medicine. In press. [PubMed] [Google Scholar]
- Seifert S. M., Seifert S. A., Schaechter J. L., et al. An analysis of energy-drink toxicity in the National Poison Data System. Clinical Toxicology. 2013;51(7):566–574. doi: 10.3109/15563650.2013.820310. [PubMed] [CrossRef] [Google Scholar]
- Caffeine-Toxicology Data Network, http://toxnet.nlm.nih.gov/cgi-bin/sis/search/a?dbs+hsdb:@term+@DOCNO+36.
- Jantos R., Stein K. M., Flechtenmacher C., Skopp G. A fatal case involving a caffeine-containing fat burner. Drug Testing and Analysis. 2013;5(9-10):773–776. doi: 10.1002/dta.1485. [PubMed] [CrossRef] [Google Scholar]
- Thelander G., Jönsson A. K., Personne M., Forsberg G. S., Lundqvist K. M., Ahlner J. Caffeine fatalities—do sales restrictions prevent intentional intoxications. Clinical Toxicology. 2010;48(4):354–358. doi: 10.3109/15563650903586752. [PubMed] [CrossRef] [Google Scholar]
- Israelit S., Strizevsky A., Raviv B. ST elevation myocardial infarction in a young patient after ingestion of caffeinated energy drink and ecstasy. World Journal of Emergency Medicine. 2012;3(4):305–307. doi: 10.5847/wjem.j.issn.1920-8642.2012.04.012. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Berger A. J., Alford K. Cardiac arrest in a young man following excess consumption of caffeinated ‘energy drinks’ Medical Journal of Australia. 2009;190(1):41–43. [PubMed] [Google Scholar]
- Scott M. J., El-Hassan M., Khan A. A. Myocardial infarction in a young adult following the consumption of a caffeinated energy drink. BMJ Case Reports. 2011;2011 doi: 10.1136/bcr.02.2011.3854.bcr0220113854 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Reis J. P., Loria C. M., Steffen L. M., et al. Coffee, decaffeinated coffee, caffeine, and tea consumption in young adulthood and atherosclerosis later in life: the CARDIA study. Arteriosclerosis, Thrombosis, and Vascular Biology. 2010;30(10):2059–2066. doi: 10.1161/atvbaha.110.208280. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Worthley M. I., Prabhu A., de Sciscio P., Schultz C., Sanders P., Willoughby S. R. Detrimental effects of energy drink consumption on platelet and endothelial function. The American Journal of Medicine. 2010;123(2):184–187. doi: 10.1016/j.amjmed.2009.09.013. [PubMed] [CrossRef] [Google Scholar]
Articles from Case Reports in Emergency Medicine are provided here courtesy of Hindawi Limited
Copyright and License Information
Copyright © 2015 Daniel Solomin et al.This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.